What is vitrification?
Vitrification is a process that has been used in the Sanatorium Helios for many years to freeze eggs and embryos. We were one of the first in Europe to routinely implement the vitrification methods already in 2006, thanks to our cooperation with GENEA, replacing the old and less successful method of slow freezing. During vitrification, the egg or embryo is placed in a special solution rich in cryoprotectants, which, together with a very rapid decrease in temperature, prevents the formation of ice crystals and thus cell damage.
Access to the latest technologies, their continuous improvement and more than 25 years of experience is the basis of your successful treatment with us. Thanks to perfect vitrification techniques, we were able to change the progress of the IVF treatment cycle and limit the transfer of fresh embryos in the post-stimulation cycle.
Hormonal stimulation, which leads to collection of more eggs and embryos from one cycle, can negatively affect the quality of the endometrium (uterine mucosa) and embryo implantation. Therefore, since 2010, we tend to decrease the number of fresh transfers and prefer cryoembryotransfer – ie transfers of thawed embryos in one of the cycles following to stimulation.
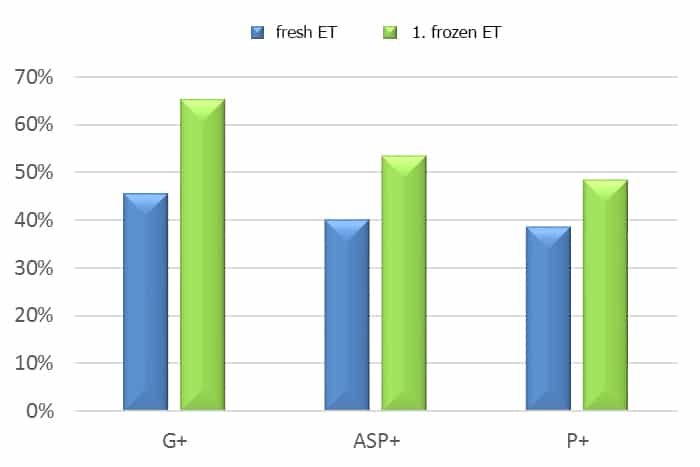
On the chart above, there is a comparison of the success rate of fresh tranfers and 1st frozen embryo transfers – G+ is a positive pregnancy test, ASP+ clinical pregnancy demonstrated by fetal heartbeat, P+ delivery.
What are the reasons for embryo vitrification?
- natural cycle transfer is preferred
- we get more than one quality embryo – blastocyst for use
- a PGT embryo examination is planned
- for health reasons fresh transfer is not recommended (polyp, risk of OHSS)
- as with eggs, it is possible to preserve embryos even before radiotherapy or chemotherapy, where there is a risk of damage to the germ cells, which leads to subsequent fertility disorder
- for example, partners plan to leave after stimulation or the patient becomes ill
What vitrification methods do we use?
We keep improving the vitrification techniques, today we have been using the 4th generation of vitrification techniques – the GAVI vitrification automat. Transfers of embryos vitrified to GAVI have 14.2 % more biochemical pregnancies and 21% more clinical pregnancies with fetal heart activity + compared to Cryotop (our results from 2016-2019 presented at the international conference Fertility Vision 2019).
